

Big Pharma, Anti-Depressants and Suicide : A Well Thought Out Scream by James Riordan

 By now it has become clear that the goal of the major pharmaceutical companies is to have every single person in America, if not the world, on some form of anti-depressant drug. Unfortunately, the AMA (American Medical Association) seems to be fully supportive of this idea. Sometimes it feels like there is only one type of drug the doctors prescribe. The kicker is that once you start taking an anti-depressant it is not recommended that you ever stop. In fact, those who do stop are very prone to serious depression and sometimes even suicide. United States health authorities recently announced that there has been a sharp increase in suicide rates since the year 2000 and called for a more thorough approach to handling depression. This news was revealed the same week as the highly publicized suicides of celebrities Anthony Bourdain and Kate Spade. Researchers admit that detailed studies in this difficult area have largely been abandoned by the major pharmaceutical companies.
By now it has become clear that the goal of the major pharmaceutical companies is to have every single person in America, if not the world, on some form of anti-depressant drug. Unfortunately, the AMA (American Medical Association) seems to be fully supportive of this idea. Sometimes it feels like there is only one type of drug the doctors prescribe. The kicker is that once you start taking an anti-depressant it is not recommended that you ever stop. In fact, those who do stop are very prone to serious depression and sometimes even suicide. United States health authorities recently announced that there has been a sharp increase in suicide rates since the year 2000 and called for a more thorough approach to handling depression. This news was revealed the same week as the highly publicized suicides of celebrities Anthony Bourdain and Kate Spade. Researchers admit that detailed studies in this difficult area have largely been abandoned by the major pharmaceutical companies.
Most antidepressants, the big names like Prozac, Zoloft, and Celexa, are classified as selective serotonin reuptake inhibitors (SSRIs). The FDA (Food & Drug Administration) admitted in 2007 that SSRIs can cause madness at all ages and that the drugs are very dangerous; otherwise daily monitoring wouldn’t be needed: “Families and caregivers of patients should be advised to look for the emergence of such symptoms on a day-to-day basis, since changes may be abrupt” … “All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases. The following symptoms, anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania, have been reported in adult and pediatric patients being treated with SSRIs. These drugs work via the hormone serotonin, often referred to as the “happiness hormone,” to increase the levels in your brain by stopping (inhibiting) the absorption (reuptake) through the brain’s various receptors.
SSRIs don’t cure depression. They can only treat the symptoms, which, in this case, are hormonal imbalances. They’re also imperfect. Dr. Ann Blake Tracy, an expert on the flaws of drugs like Prozac and Zoloft, points out in her book Prozac: Panacea or Pandora? that “animal studies demonstrate that in the initial administration Prozac actually causes the brain to shut down its own production of serotonin, thereby causing a paradoxical effect or opposite effect on the level of serotonin.” The brain’s chemistry naturally wants to remain balanced, she adds, and any disruption from SSRIs or other medications throws that balance off.
What results from this volatility is something like a rollercoaster effect. A person’s mood goes from consistently depressed to temporarily content to all over the place very quickly. It’s for this reason the Food and Drug Administration requires “Black box warnings” on all SSRIs, stating explicitly that they double suicide rates from two per 1,000 to four per 1,000 in children and adolescents.
Another theory claims that antidepressants aren’t directly increasing a person’s risk at all. SSRIs endow depressed people with a newfound alertness and proactivity. If someone was suicidal before taking an antidepressant, but unmotivated to act on their urge, the antidepressant only facilitated their latent desires; it didn’t create them. In both cases, a 2004 study argues that it’s within the first nine days of taking antidepressants a person is most at-risk for suicidal thoughts or behaviors.
 The medical community tells you that you’ll be calmer and happier when you are taking these drugs. They do warn you that possible side effects are drowsiness, nausea, dry mouth, insomnia, diarrhea, nervousness, agitation or restlessness, dizziness and sexual problems, such as reduced sexual desire or difficulty reaching orgasm or inability to maintain an erection (erectile dysfunction). So, say you are tired being dizzy and having diarrhea – well they’ll just switch you to a similar drug and hope the side effects stop. If they persist they’ll run you through the gamut of such drugs, all the while emphasizing that you cannot stop taking them. What happens many, many times is that people just get fed up with this drug dance and stop taking their medication. Then, they get depressed. After that, most got back to the doctor, especially those patients who have someone in their lives who care about them and notice they are sliding down the chute to clinical depression. Others are not so fortunate. A recent study in Great Britain showed conclusively that antidepressants can raise the risk of suicide. An analysis of 70 trials of the most common antidepressants – involving more than 18,000 people – found they doubled the risk of suicide and aggressive behaviour in under 18s. The review accused pharmaceutical companies of failing to report side-effects and even deaths linked to the drugs. Although a similarly stark link was not seen in adults, the authors said misreporting of trial data could have led to a ‘serious underestimation of the harms.’
The medical community tells you that you’ll be calmer and happier when you are taking these drugs. They do warn you that possible side effects are drowsiness, nausea, dry mouth, insomnia, diarrhea, nervousness, agitation or restlessness, dizziness and sexual problems, such as reduced sexual desire or difficulty reaching orgasm or inability to maintain an erection (erectile dysfunction). So, say you are tired being dizzy and having diarrhea – well they’ll just switch you to a similar drug and hope the side effects stop. If they persist they’ll run you through the gamut of such drugs, all the while emphasizing that you cannot stop taking them. What happens many, many times is that people just get fed up with this drug dance and stop taking their medication. Then, they get depressed. After that, most got back to the doctor, especially those patients who have someone in their lives who care about them and notice they are sliding down the chute to clinical depression. Others are not so fortunate. A recent study in Great Britain showed conclusively that antidepressants can raise the risk of suicide. An analysis of 70 trials of the most common antidepressants – involving more than 18,000 people – found they doubled the risk of suicide and aggressive behaviour in under 18s. The review accused pharmaceutical companies of failing to report side-effects and even deaths linked to the drugs. Although a similarly stark link was not seen in adults, the authors said misreporting of trial data could have led to a ‘serious underestimation of the harms.’
For years families have claimed that antidepressant medication drove their loved ones to commit suicide, but have been continually dismissed by medical companies and doctors who claimed a link was unproven. The review – the biggest oif its kind into the effects of the drugs – was carried out by the Nordic Cochrane Centre and analysed by University College London (UCL) who today endorse the findings in an editorial in the British Medical Journal (BMJ). After comparing clinical trial information to actual patient reports the scientists found pharmaceutical companies had regularly misclassified deaths and suicidal events in people taking anti-depressants to “favour their products”.
The fine print at the bottom of prescription drug commercials may provide ample comedic firepower — what are they hiding? — but underneath the humor lies a chilling reality: In their noble pursuit of making you healthy, prescription drugs put you at risk for a number of terrifying side effects, chief among them being antidepressants’ risk for suicide.
Where would we be without medication? The Centers for Disease Control and Prevention reports nearly half of the U.S. population has used at least one prescription drug within the last month, with drugs ordered or provided during physician office visits totaling 2.6 billion in 2010. Antidepressants alone, which have been derided as overprescribed, are used by more than 10 percent of the population 12 years and older. Among women in their forties and fifties, the rate jumps to 25 percent.Do
In pharmacology, this overall effect is known as a “paradoxical reaction.” A specific medication was intended to treat one symptom, but ended up producing it in greater magnitude. Benzodiazepines, common psychoactive drugs used to relax muscles and quiet convulsions, are prone to producing the exact opposite effects. Antibiotics as well, which have been in greater circulation in recent years, have been known to produce the “Eagle effect” — a phenomenon named after Harry Eagle, the physician who first noticed that when bacteria are exposed to antibiotics for a long enough time, their population rates not only stabilize; they increase.
Paradoxical reactions have been observed in depression sufferers and also obsessive-compulsive disorder sufferers. A 1990 study showed 10- to 17-year-olds were compelled to self-harm following administration of fluoxetine (Prozac), leading to the hospitalization of four out of the 42. And while certifiable advances have been made in the 24 years following the study, SSRIs continue to carry the warning. They have to: As long as the medication that’s designed to realign the juices in our brain that make us happy or depressed can turn against us, the threat of ending it all will always be lurking in the fine print.
 Robin Williams, Chris Cornell, and Chester Bennington all revealed details of their struggles with depression and anxiety before they made the tragic decisions to end their lives. You’re probably not surprised that people diagnosed with a psychiatric disorder, such as depression or anxiety, have an increased risk of suicide; in fact, a recent study estimates that 80% of people who attempt suicide have a psychiatric diagnosis associated with suicidal ideation. The startling news comes from the science that supports the causal role of antidepressants in the actual completion of suicide.
Robin Williams, Chris Cornell, and Chester Bennington all revealed details of their struggles with depression and anxiety before they made the tragic decisions to end their lives. You’re probably not surprised that people diagnosed with a psychiatric disorder, such as depression or anxiety, have an increased risk of suicide; in fact, a recent study estimates that 80% of people who attempt suicide have a psychiatric diagnosis associated with suicidal ideation. The startling news comes from the science that supports the causal role of antidepressants in the actual completion of suicide.
If depression leads to suicide and antidepressants like SSRIs resolve depression, we could decrease suicide rates by increasing the number of antidepressant prescriptions, right? That’s the pharmaceutical argument for medicating people who are “at risk”.
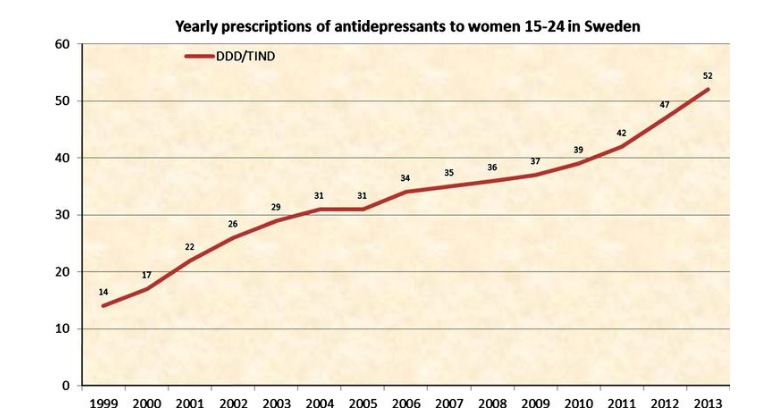
Yet, the evidence reveals some inconvenient truths, demonstrating that antidepressants actually increase the risk of suicide. Furthermore, just as the serotonin model of depression has never been scientifically validated, there is no evidence that antidepressants meaningfully and statistically significantly resolve depression – but, instead, we are confronting a growing signal of harm, including live-streamed suicides and school shootings committed by those recently prescribed. And a new study from Sweden that examines antidepressants in the context of suicide suggests that antidepressants are pushing people towards, not away from, suicide.
Swedish researchers analyzed data in a timespan in which antidepressant prescriptions rose steadily; the percentage of young women who were prescribed antidepressants increased from 1.4% to 5%. Approximately 500 young women committed suicide during this time period, and because toxicological analyses were performed postmortem, researchers could determine if these women were on antidepressants at the time that they made the decision to end their lives.
If antidepressants indeed resolve depression and prevent suicide, those who committed suicide, would be the unmedicated ones right? Also, suicide rates would decrease as antidepressant prescriptions increased.
Yet, researchers found the opposite. As antidepressant prescriptions increased 270% over 15 years, suicide rates also increased. Strikingly, more than half of the young women who committed suicide (52%) were prescribed antidepressants within a year of committing suicide. And antidepressants were detected in 41% of the women who committed suicide, showing that they were under the influence of antidepressants at the time of death. In the remaining subjects, it is also important to know whether they had recently discontinued psychotropic medication. As many who have done so would tell you, abrupt (or sometimes even cautious) tapering of medication can lead to suicidality and homicidality with associated impulsivity (long after the medication itself is undetectable).
We are a culture that believes that force is necessary for change and progress (rather than natural momentum and emergent processes). But maybe we shouldn’t be surprised when we learn that throwing more of the same failed medicine at the very problem created by the failed medicine – well, it doesn’t actually work. Herein lies the thinly-veiled agenda of the industry – use the shortcomings of the intervention (in this case, continued and worsened depressive symptoms) to justify further interventions (more medications for all). This is like calling for more and more barricades to cover up any visual evidence of a forest fire while the fire blazes behind the facade. What is needed, at the first sign of risk outweighing benefit, is true informed consent – and thankfully, each and every prospective patient can now be empowered with a fuller version of the truth than they might receive from media, the government, or their prescribing doctor.
Regarding the British study, experts said the review’s findings were “startling” and said it was “deeply worrying” that clinical trials appear to have been misreported. Dr Joanna Moncrieff from University College London said: “People in the United Kingdom are consuming more than four times as many antidepressants as they did two decades ago. Despite this, we still do not fully understand the effects of these drugs.”
The UK now has the seventh highest prescribing rate for antidepressants in the Western world, with around four million Britons taking them each year – twice as many as a decade ago at a cost of more than £200 million a year for the 53 million prescriptions now written.
 Although NHS guidelines state that under 18s should not be given antidepressants there are more than 100,000 prescriptions for Prozac each year for teenagers, despite reviews showing that the drugs are no more effective than counselling.
Although NHS guidelines state that under 18s should not be given antidepressants there are more than 100,000 prescriptions for Prozac each year for teenagers, despite reviews showing that the drugs are no more effective than counselling.
The review looked at the five most common drugs prescribed for depression in Britain – including Prozac. It analysed the published summary reports provided by pharmaceutical companies to drugs regulators and compared it with the raw data from clinical trials. Tarang Sharma of the Nordic Cochrane Centre, Copenhagen, Denmark admitted: “The analysis suggests that clinical study reports, on which decisions about market authorisation are based, are likely to underestimate the extent of drug related harms.”
Four deaths were misreported by one unnamed pharmaceutical company, who claimed they had occurred after the trials had stopped.
One patient strangled himself unexpectedly after taking venlafaxine but because he survived for five days, he was excluded from the results because it was claimed he was no longer on the trial while he was dying in hospital.
More than half of the suicide attempts and suicidal thoughts had been misrecorded as emotional instability or worsening of depression. In summary trial reports from the drugs giant Eli Lilly, suicidal attempts were missing in 90 per cent of cases.
One father whose son committed suicide after taking Citalopram has been monitoring suicides related to antidepressant medication for the last three years and has set up the anonymous campaigning website AntiDepAware.
So far this month there have been at least 35 inquests with deaths linked to antidepressants. Last year there were more than 450.
A father whose son committed suicide said, “I can say, hand on heart, that I don’t remember reading a report of an inquest where a suicide verdict was applied to a child who had never been on any psychiatric medication,” he said.
Professor Peter Gøtzsche, the lead author from the Nordic Cochrane Centre said: “Antidepressants don’t work in children, that is pretty clear, in the randomised trials children say that they don’t work for them, but they increase their risk of suicide. “What I get out of this colossal underreporting of suicides is that SSRIs likely increase suicides in all ages.”
The authors concluded that that exercise and psychotherapy should be offered to children and young adults before anti-depressants because that harms are likely to outweigh the benefits. The drugs which reviewed were duloxetine, fluoxetine – which is also known as Prozac – paroxetine, sertraline and venlafaxine which belong to two classes, Selective serotonin reuptake inhibitors antidepressants (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs). Commenting on the findings of the review Professor Gotzsche added, “It is absolutely horrendous that they have such disregard for human lives.”
Lucie Russell, Director of Campaigns for YoungMinds: “This new study is deeply worrying, and it’s very concerning that some clinical trials have been misreported or poorly designed. “Children and their parents must have solid and comprehensive information about the effects that antidepressants can have so they can make informed decisions about treatment. “We believe that prescribing antidepressants should never be the only course of action.”
Marjorie Wallace, Chief Executive of the mental health charity SANE added: “This new report indicates that great caution must be taken in prescribing new-generation anti-depressants (SSRIs) for children and adolescents.”
Health experts said misreporting of trial data was a growing problem. Dr Paul Ramchandani, Consultant Child and Adolescent Psychiatrist with Central North West London Foundation NHS Trust said: “There have been concerns for a number of years about the way in which some trials of medicines or drugs for depression were originally reported, particularly when the treatment was for children and adolescents.”
Dr Paul Keedwell, Consultant Psychiatrist and Senior Research Fellow in the Neurobiology of Mood Disorders at Cardiff University, added:“The findings provide a further lesson in how professionals must carefully scrutinise drug company summaries for data on adverse events.”
However drug companies defended their data, saying that safety was their top priority. A spokesman for Eli Lilly said: “No regulatory authority has ever determined that Lilly withheld or improperly disclosed any data related to these medications. “Put simply, our goal is to make life better for people around the world, and Lilly is committed to sharing the results of our clinical trials and ensuring this information is available to the people who need it.”
After my 16 year old son was killed as a passenger where three drunk drivers were involved, people told me I should start taking anti-depressants. My response was that I had a reason to be depressed, at least for a while anyway. I had just lost my son, who was one of the most remarkable human beings I ever knew. I had thought that anti-depressants were for people who were unreasonably depressed, but I soon learned that no, they are for everyone who is not happy. I think that includes almost every person on the planet.



{kind=link}
No Comment